Breast Cancer

Snapshot
~2.3 million new cases per year worldwide — it's not rare, it's the most common cancer in women. About 70% are hormone receptor-positive, meaning they depend on oestrogen to grow. Catch it at Stage I and over 95% of patients survive 5 years. Miss it until Stage IV and that number drops to 28%. The practical message: screen early, biopsy definitively, and always check the receptor status before touching treatment.
Molecular Subtypes
Breast cancer is not one disease. The four molecular subtypes behave completely differently — different prognosis, different treatment. The subtype is defined by three immunohistochemistry markers: ER, PR, HER2. Know these cards cold.
Clinical Presentation
Most breast cancers are found on routine screening — the patient feels completely well. When symptoms do appear, think in terms of what the tumour is doing to nearby structures.
- Painless lump — firm, irregular, poorly mobile. Upper outer quadrant (UOQ) most common. Pain is a late or unusual feature.
- Skin dimpling — Cooper's ligaments tethered by the tumour. Pathognomonic when present.
- Peau d'orange — orange-peel texture from dermal lymphatic blockage. Suggests locally advanced disease.
- Nipple changes — retraction, bloody/serous discharge, inversion in a previously normal nipple.
- Paget's disease — eczematous, crusting nipple rash. Always underlying DCIS or invasive cancer. Biopsy the nipple, don't treat as eczema.
- Inflammatory breast cancer — diffuse erythema, warmth, rapid onset, no fever. Looks like mastitis but isn't. Core biopsy urgently.
- Axillary nodes — hard, fixed ipsilateral nodes suggest nodal spread.
A young woman presents with a red, swollen breast unresponsive to antibiotics. Think inflammatory breast cancer, not mastitis. The key differentiator: inflammatory BC has no fever, no leukocytosis, and doesn't improve with antibiotics. Punch biopsy of the skin is the next step.
Diagnostics & Staging
All three are required. A positive clinical exam alone or positive mammogram alone is not enough to treat. You need tissue.
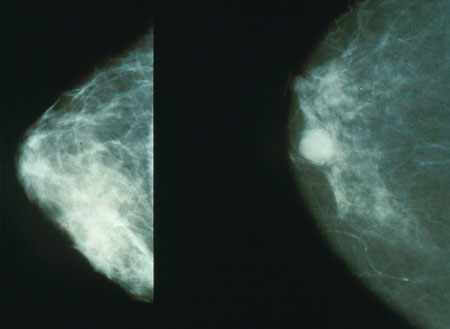
- MammographyFirst-line imaging. Look for: spiculated mass, microcalcifications (DCIS), architectural distortion, asymmetry.
- UltrasoundFor dense breasts, women <35, axillary nodes. Distinguishes solid vs cystic. Guides biopsy.
- Core needle biopsyGold standard. Gives histology + grade + ER/PR/HER2/Ki-67. Must be done before any treatment decision.
- MRI breastHigh-risk surveillance (BRCA+), lobular cancer extent assessment, pre-op planning. Not routine.
- Staging CT + bone scanFor Stage III–IV or symptoms (bone pain, cough, dyspnoea, neurological). PET-CT increasingly preferred.

TNM Staging & Survival
| Stage | Description | 5-yr Survival | Prognosis |
|---|---|---|---|
| 0 | DCIS — non-invasive, confined to ducts | ~99% | Excellent |
| I | Tumour ≤2 cm, node-negative | >95% | Excellent |
| II | Tumour 2–5 cm or 1–3 positive nodes | ~86% | Good |
| III | Large tumour, ≥4 nodes, skin/chest wall involvement | ~57% | Fair |
| IV | Distant metastases — bone, lung, liver, brain | ~28% | Poor |
Management
Treatment is multimodal and always subtype-driven. The biopsy report — especially ER, PR, HER2, and Ki-67 — determines the systemic therapy before surgery is even discussed. The sequence below applies to early-stage (I–III) disease.
- Survival equivalent to mastectomy for Stage I–II — offer this first
- Radiotherapy is mandatory post-BCS — reduces recurrence by ~50%
- Requires clear surgical margins (≥1 mm)
- Not suitable if: multifocal, large tumour-to-breast ratio, prior chest RT
- Large tumour (>5 cm) or poor tumour-to-breast ratio
- Multifocal or multicentric disease
- BRCA1/2 carrier — prophylactic contralateral mastectomy discussable
- Patient preference after fully informed consent
- SLNB — sentinel lymph node biopsy for all clinically N0 patients. Avoids full dissection + morbidity.
- ALND — axillary lymph node dissection if ≥3 positive sentinel nodes or clinically N+
- Lymphoedema risk rises significantly with ALND — avoid unless necessary
- Always after BCS — whole breast RT is standard of care
- Post-mastectomy if: T3/T4, ≥4 positive nodes, close/positive margins
- Regional nodal RT if axillary, internal mammary, or supraclavicular nodes involved
Metastatic breast cancer is not curable with current treatments — the goal is disease control, symptom management, and quality of life. That said, modern targeted therapies have transformed median survival from ~18 months to several years in HR+ and HER2+ disease.
Palbociclib, ribociclib, abemaciclib.
Doubles PFS vs AI alone.
Pertuzumab + trastu 1st line.
Bone mets: denosumab or bisphosphonates to prevent skeletal events.
Clinical Pearls
